What is perineotomy and when is it used in childbirth?
The generic process is very complex and largely unpredictable. And because in the course of the birth of the baby, doctors are always ready to provide any assistance to the woman. Perineotomy is one of the methods of active obstetric protection. The fact that this and why this procedure can be carried out in childbirth, we will describe in this article.
Special features
The birth of the fetal head is an important and crucial moment, which can sometimes be overshadowed by purely physical difficulties - the discrepancy between the size of the exit from the vagina and the diameter of the head, resulting in the likelihood of spontaneous rupture of the perineum. If such a rupture occurs, the consequences can be very serious - sometimes not only the genitals, but also the intestines are injured, severe bleeding, vaginal-rectal fistula develops.
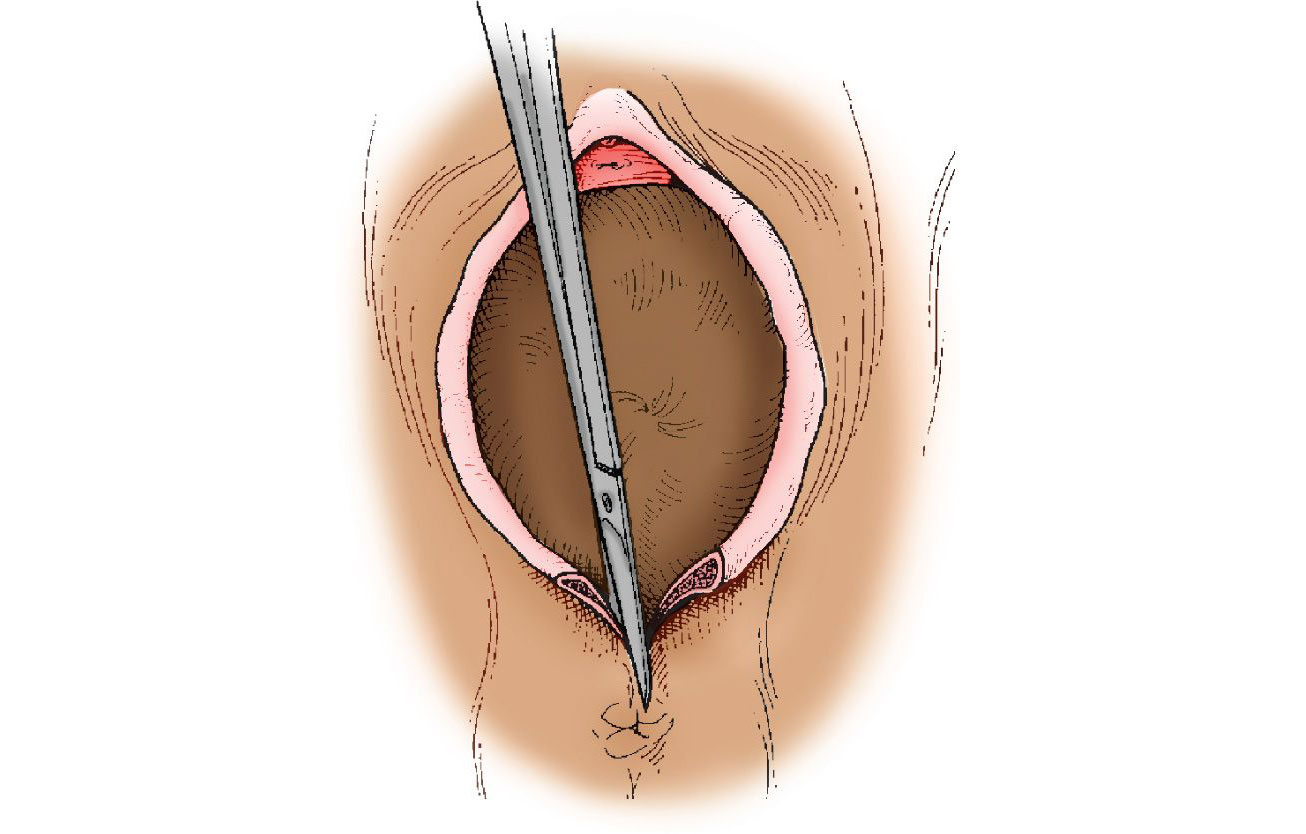
If such a delicate situation occurs, at birth, obstetricians can apply a perineotomy - surgical dissection of the perineum of the median type. With episiotomy an incision is made from the center to the right or left side, diagonally.
Perineotomy involves a smooth vertical incision, directed downward from the center of the perineum, to the anus. The length of the cut - 2-3 centimeters. This is where the main difference from episiotomy lies. The rest of the methods are no different, and therefore perineotomy is considered one of the types of episiotomy, distinguishing it in the classification of types of dissection honorable second place.

Such an artificial extension of the perineum allows the child to quickly leave the birth canal, if the situation requires, and the incision prevents tearing, which has a positive effect on recovery after birth.
The difference between episiotomy and perineotomy is almost imperceptible in the rehabilitation process, because the rules of stitching and basic recommendations for women in childbirth with a mid-lateral (diagonal) cut and a straight (middle) cut are almost the same.
The name of the manipulation comes from the Greek perineotomia (in turn, this word consists of perineos - "female perineum" and tome - "dissection"). It is used on a par with episiotomy and is a free choice of the doctor or obstetrician who takes birth. That is, the way to make the dissection is decided by the situation. Although some studies show that with a vertical midline incision there is a higher risk of continuing the gap along the notch down to the rectum. Therefore, mid-lateral dissection is considered more appropriate. But there is no clear indication of this.
Until recently, manipulation was widespread in obstetrics. "Cut" almost every woman in labor. Today, on the recommendation of the WHO and the Ministry of Health of Russia, perineotomy is used less frequently and only if there are certain indications.

Indications
As already mentioned, before the dissection was done for preventive purposes - in order to prevent ruptures of the perineum. Today, the view of perineotomy and episiotomy has changed. The Ministry of Health recommends the tactics of observation and waiting. Medical staff may resort to surgical dissection only when there is a high probability of rupture during pathological delivery.
There may be a need for a midline incision. at the birth of a large baby, with a large diameter of the head or legs born forward. Usually, under such circumstances, a cesarean section is recommended, but the woman has the full right to write a refusal and insist on natural childbirth.
If doctors need to apply forceps or a vacuum extractor, there is also a need to expand the intermediate region surgically. Colloidal and thinned, heterogeneous scars from previous gaps or incisions can also be the basis for a midline incision.
High perineum and rigidity for some time are not considered grounds for the indispensable perineotomy.
The method can be applied if a woman is forbidden for medical reasons to make a lot of pressure (for example, in case of eye diseases). Great hopes are placed on manipulation even in the case of the discovery of a state of hypoxia in a child whose head is already at the exit from the vagina.

Performance technique
An incision is made exclusively in the period of attempts, neither earlier nor later. The head should already cut through and look out about 3-4 centimeters at the peak of the next attempts. Blunt surgical scissors are taken. In the gap between attempts, one end is inserted inside, the other remains outside. At the peak of the attempt is a cut in one motion. Only skin is cut.
In order to prevent a further cut gap, it is recommended to manually control the speed of birth of the head. If the baby is in a hurry, it is held back with a little palm.
Perineotomy itself can be anesthetized topically with lidocaine, and it can be done without anesthesia, since at the peak of the attempt at skin tension the incision is almost not felt. If there is a catheter in the spinal canal and a woman in labor receives an epidural anesthesia, if necessary, they can additionally inject a little anesthetic.
After birth, the placenta is checked for the condition of the cervix, if necessary, it is sutured, and only then the delivery is completed by stitching the cut crotch. The algorithm is quite simple:
the perineum is treated with an antiseptic;
take measures for pain relief (local);
catgut threads suture the incision site, and silk surgical sutures are applied to the skin;
again spend processing antiseptic.
Subsequently, antiseptic treatments are repeated daily.

Complications
It is very difficult to handle the seams independently. The crotch zone is not the most convenient place for this. But while the woman is in the hospital, she has nothing to worry about - the treatment is carried out by medical personnel. At home, a husband can help in this matter. It is advisable to treat the wound using hydrogen peroxide and brilliant green. This will help dry it and avoid bacterial contamination.
Considering that the wound in the perineum cannot be constantly ventilated, and is in direct contact with postpartum bleeding, special attention should be paid to treatment and care, because inflammation is the most common complication of perineotomy.
Normally, silk threads are removed for 6-7 days, and complete healing in the absence of complications takes place within 3-4 weeks. With a longer healing time, when the suture is compacted, the cones appear on it, the blood of the ichor or pus is released, you should immediately consult a doctor and get the necessary treatment.
Common complications also include seam divergence. It can occur due to excessive stress on the perineum, due to violations of the requirements of the motor mode, due to flaws in obstetrics - mistakes made in the suturing technique or incorrectly selected suture set. This is manifested by the resumption of blood or bleeding from the rumen, gaping wounds at the point of divergence, increased pain and swelling.
A discrepancy may require re-suturing only when the fusion did not occur over most of the incision length. In other cases, doctors clean the wound, disinfect it and recommend local anti-inflammatory or antibacterial agents (“Levomekol", eg). Healing occurs by secondary intention.
Inflammation and suppuration require treatment with antibiotics, and the formation of hernias, fistulas, internal hematomas requires surgical care.
Complaints of a woman that at first she hurts her to stand and walk is not considered a complication - while the nerve endings and the integrity of the skin are being restored, the discomfort and pulling pain are normal.

When can I sit down? Seam care
The first thing that puerperas after perineotomy usually interests is whether you can sit. You can not sit. If, after a mid-lateral incision, you can sit down with one hip, in order to relieve the tension of the perineum, it is not recommended to sit after the mid-vertical incision. Walk with caution, without making sudden movements. To feed the newborn - standing or lying down, and to eat and drink tea - while standing.
If the stitches heal without significant problems and complications, then a woman can sit down after about three weeks. If there are complications, then the period of prohibition of such a posture can be individually increased over time.
During discharge, a woman should be placed in the back seat of a car lying on her side, so as not to accidentally damage the crotch seams on the way.
The following recommendations will help to avoid unpleasant consequences and speed up healing:
change the gasket as often as possible;
after visiting the toilet you need to wash;
wipe the crotch is not necessary, you should only gently and gently soak it with a soft cloth or a separate diaper allocated for this;
once a day the crotch should be left open for half an hour for ventilation and drying;
you can not take a bath until the wound heals after perineotomy, you can only wash in the shower;
If problems are found, you need to contact a gynecologist.
After healing, that is, in the second month after childbirth, a woman can begin to use a tool that increases the elasticity of scars by increasing the amount of collagen - “Contractubex».
It is recommended to conduct a sexual life not earlier than postpartum discharge. In the first six months after childbirth, due to the presence of a scar, a woman may experience discomfort during intimacy. Gradually they will pass, such a phenomenon does not need treatment.






