Epidural anesthesia during childbirth

Modern mothers are more fortunate than their mothers and grandmothers. Medicine is ready to offer them effective ways to reduce birth pain. One of such methods is epidural anesthesia, which is quite widely used both during physiological labor and during surgical delivery.
This article will discuss how such anesthesia is done, what its advantages and disadvantages are and whether it can have negative consequences.


What it is?
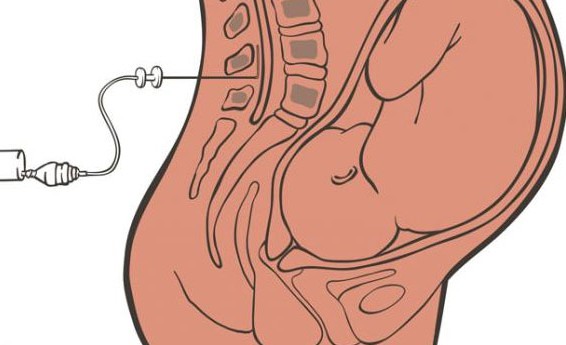
Peridural or epidural anesthesia - a method of gentle anesthesia. In order to alleviate the pain, the patient does not need to be completely immersed in a medication sleep. The woman remains conscious, but an epidural injection into the spine deprives, in whole or in part, her susceptibility in some parts of the body.
The spine is part of the central nervous system, there are numerous endings of the nerve processes that send impulse signals to the brain. This is how the signal of pain is transmitted. The pain center in the cerebral cortex takes it, analyzes it, and the person begins to feel pain.
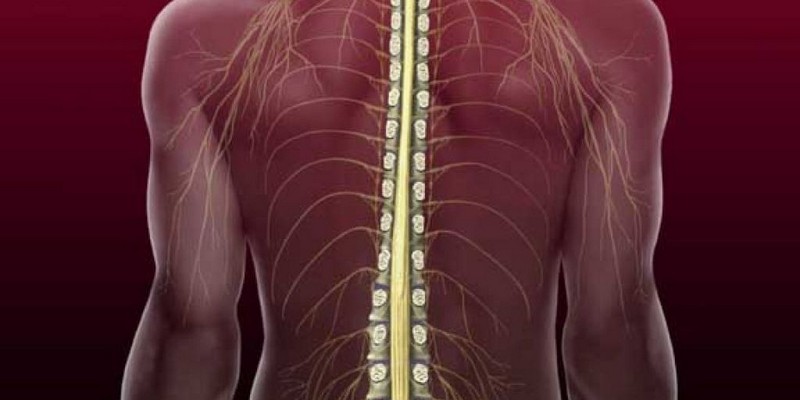
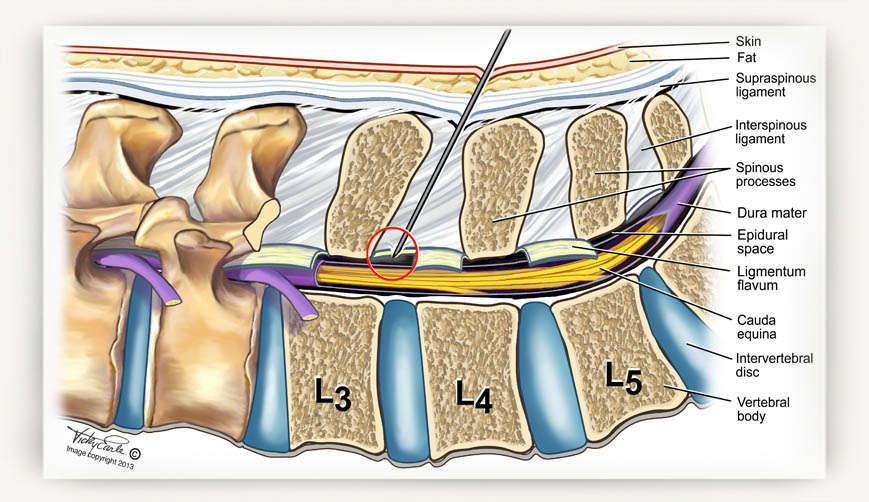
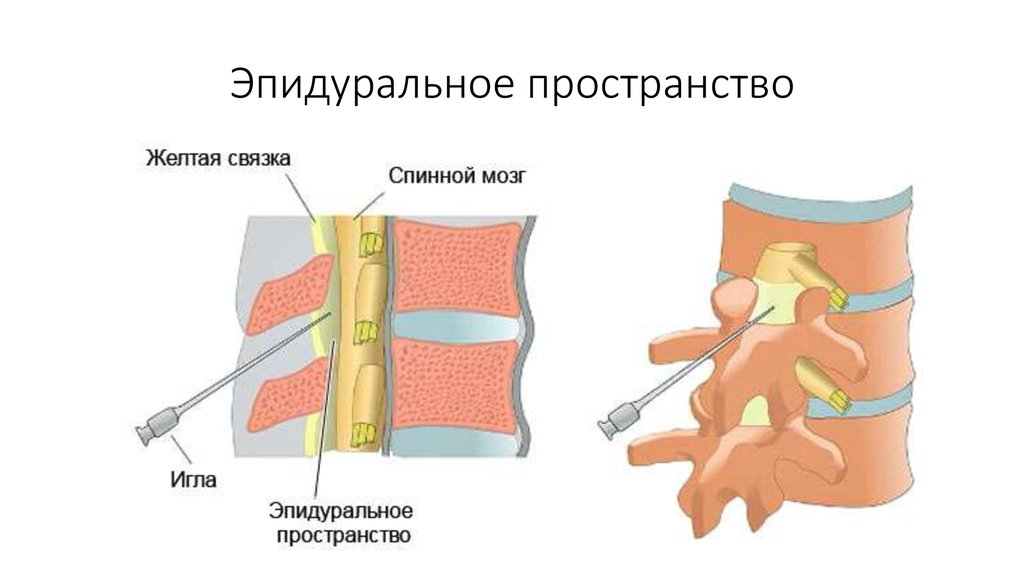
The technique of epidural anesthesia lies in the fact that it is in the spine, or rather, in its epidural space, with the help of a long lumbar needle and a catheter medications are injected that block the sending of a pain impulse. As a result, the brain simply does not accept and does not understand the signals from certain nerve endings. For anesthesia of different parts of the body, the drugs are injected into different parts of the spinal column.
In labor and surgical delivery, there is a need to desensitize the lower body, and therefore an injection is made in the lumbar spine.
The nerve roots are washed by the drug - an anesthetic inserted through a catheter, their sensitivity is temporarily dulled or disappears altogether. For vaginal delivery, drugs and dosages are used other than caesarean section. A woman who gives birth by herself, thus gets the opportunity to relive the pain of birth, but does not completely reduce the sensitivity, she feels the lower part of the body.
For caesarean section, there is a need for a longer and deeper anesthesia, therefore, not only analgesics, as in the first case, are administered, but also ketamine.
Preparations that are used for epidural anesthesia undergo a special specific cleaning, the resulting solutions are intended only for spinal or epidural use. What drug to enter and in what quantity, knows the anesthesiologist. He is repelled not so much by the weight of a woman as by her height.
Taken on each segment of the spinal column that needs to be anesthetized, apply up to 2 ml of medication. Plays the role and the general condition of the woman, her pain threshold, the individual characteristics of her health.

Advantages and disadvantages
Analgesia through the introduction of pain medication into the epidural space is considered to be a fairly safe method today; therefore, the Ministry of Health recommended it as a first-line solution in situations where local anesthesia during childbirth or deeper anesthesia as an alternative to general anesthesia is necessary for surgery.
All the pros and cons of this type of pain reduction should be taken into account by two specialists - the doctor who is giving birth or operates and the doctor-anesthesiologist. They must take into account the wishes of the woman in labor.
Thus, a woman can always refuse an epidural injection during labor or declare her disagreement with this method of anesthesia before a cesarean section. In this case, alternative methods will be used, which we describe below.
The undoubted plus of epidural pain relief is that it helps a woman to relive difficult moments more easily. When a cesarean woman maintains clarity of consciousness and can see how her baby is born. The exit from such anesthesia is incomparably shorter and easier than the exit from general anesthesia. The disadvantages are that epidural anesthesia can be harmful.

Aggravating consequences after the use of such anesthesia during childbirth may consist in lengthening the period of childbirth, weakening contractions, which can be dangerous for the child and the mother.
Complications, according to statistics, are not as common - in about one case per 50,000 births. Approximately 15-17% of women in labor, peridural anesthesia does not work as we would like - the necessary degree of anesthesia cannot be achieved, which means that the pain susceptibility is partially preserved, which makes it difficult for surgeons and obstetricians.
Epidural anesthesia can have negative consequences for women with problems with hemostasis. A violation of blood clotting can lead to the formation of hematomas in the puncture area with a small amount of blood entering the cerebrospinal fluid.

If anesthesia is performed by an experienced doctor, there’s nothing to worry about. He without significant difficulties will be able to determine the exact puncture site and the rate of drug administration. But a negligent and inept physician can injure hard spinal membranes, which is fraught with leaks of cerebral fluid, CNS dysfunction. If the needle goes deeper than necessary and injures the subarachnoid space of the spine, the woman may experience convulsions, and she may lose consciousness. In severe cases, paralysis occurs.
After applying this method of reducing pain, women often have a headache, and these pains can last up to several months. Most of them pass on their own with time.

The harm to the child from the action of drugs is almost equivalent to that of general anesthesia. In some cases, there is a risk of disturbed heartbeat and oxygen starvation and respiratory failure after the baby is born.
Contrary to popular belief that anesthesia is a serious burden on the heart, doctors say that the heart and blood vessels of the woman who was given an anesthetic by the lumbar puncture are working normally and steadily.
For many pregnant women, this method of reducing pain causes fear. Psychologically, it is difficult to accept the fact of injection into the spine. The hardest thing for those who show surgical childbirth. Not every pregnant woman is ready to see all the stages of her own operation.

Who is contraindicated?
No woman can give epidural anesthesia if she categorically objects to this. Therefore, the main contraindication is considered to be the patient’s own desire. If a woman believes that she can cope with labor contractions herself or prefers to lie on the operating table under general anesthesia, she only needs to sign the appropriate waiver.
But there are women who just want to be helped in this way. And here you can meet certain obstacles that will not allow doctors to do epidural anesthesia. Absolute contraindications include:
- patient's disagreement;
- the presence of purulent inflammation, pustules and purulent rash on the back in the area of the intended puncture;
- coagulopathy (especially against the background of severe forms of preeclampsia).
Relative contraindications to epidural anesthesia are:
- diseases of the nervous system of women, especially those associated with dysfunction of the spine;
- tattoos at the site of the intended puncture;
- deformational changes of the back, spinal injuries (with injuries in the lumbar region, the prick is most likely to be denied);
- hemorrhage (pathological hemorrhages in different parts of the body);
- systemic sepsis in the parturient woman;
- high risk of distress syndrome in the fetus (in preterm labor, when the lung tissue of the fetus is not fully matured).

According to relative indications, women with a high degree of obesity may also refuse. Epidural anesthesia will not be performed if the second birth proceeds with a scar on the uterus - anesthesia may make the symptoms of uterine rupture completely invisible if it occurs.
Do not make such an anesthesia for women who have opened bleeding, as well as in the event that childbirth takes place on the background of lowering blood pressure, dehydration.
Peridural anesthesia can also be dangerous in cases of acute hypoxia of the fetus. If something went wrong in the generic process, complications began and other obstetric response measures had no effect, the decision was made to conduct an emergency cesarean section. In this case, the woman does only general anesthesia. General anesthesia is also recommended if additional surgical intervention is needed, for example, removal of the uterus after cesarean.
For women with heart failure and pacemakers, such anesthesia can only be performed with the permission of a cardiac surgeon. If there is no such specialist and permission has not been obtained in advance, the introduction of painkillers into the spine may be denied.


Alternatives
If a woman is contraindicated for some reason with epidural anesthesia, this does not mean that she will have to endure severe pain. When carrying out artificial labor (cesarean), a woman will undergo general anesthesia, in which there are no contraindications in principle. In this case, an anesthetic will be injected intravenously, and after such an injection the patient will just fall asleep. She will not feel the anesthesiologist insert the tracheal tube into the trachea and connect it to the ventilator.
The degree of pain blockade with this method is very high.

Spinal anesthesia, in which the introduction of drugs is carried out to a deeper level - the level of the subarachnoid space of the spinal column, cannot be considered as an alternative, since the same list of contraindications works for it.
To reduce pain during physiological labor, intravenous injections of systemic anesthetic drugs can be used.

With physiological childbirth
Special preparation requires only epidural anesthesia, which is planned for caesarean section. This is a standard preparation for the operation and sedation (sedatives and hypnotic drugs before the planned operation). If there is a need to do an epidural anesthesia during labor, no preparation is required.
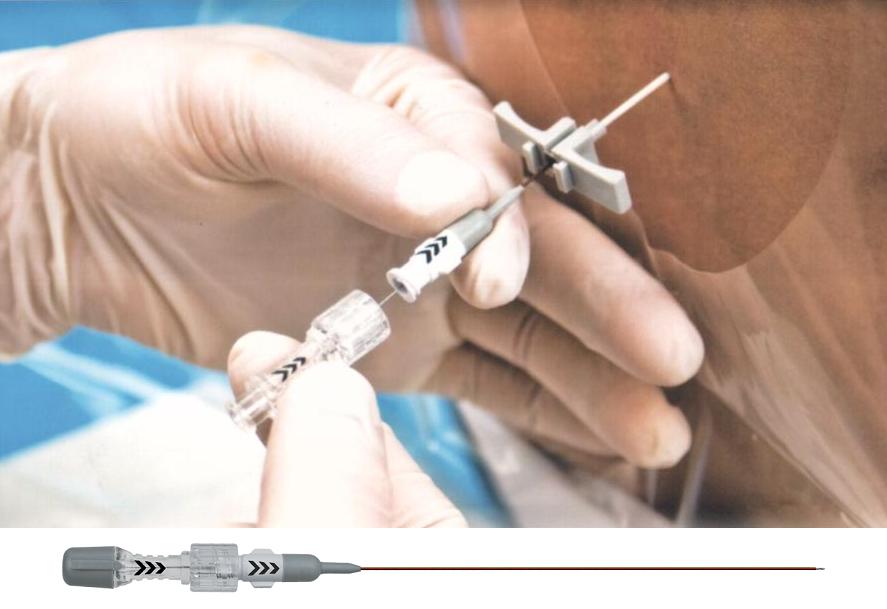
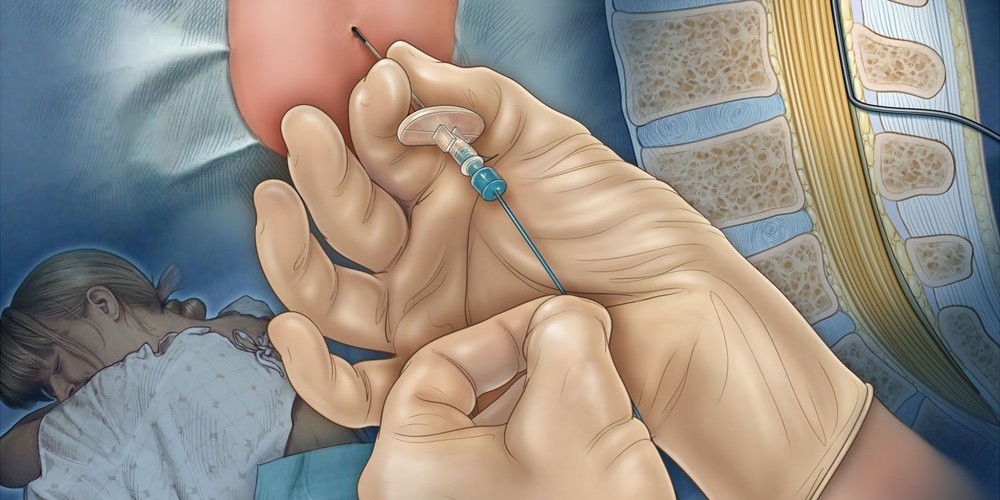
The woman is placed either in the supine position with her legs, or in a sitting position with her back arched. After that, the doctor conducts aseptic treatment of the skin area and proceeds to determine the point of injection. Usually, to reduce pain during contractions, a needle is inserted between the first and second lumbar vertebrae. The needle size 16-18G is inserted in the sagittal plane.

Once in the epidural space, the doctor will feel the needle “fail” and the lack of resistance with further advancement of the catheter. After the aspiration test, the first test dose of the drugs is injected (usually Lidocaine or Bupivacaine is used). The catheter remains at the puncture site.If necessary, medication can be added through it if the woman begins to feel pain again. Therefore, she cannot lie on her back. Contractions will occur in the supine position on the right or left side, you need to change the side every hour.
Anesthesia begins to act within 15-20 minutes after drug administration. The duration of anesthesia may be different, it depends on the dosage. Often, during natural births, doctors use a technique in which the patient adjusts the dosage herself - when pain occurs, she lets the anesthesiologist know this, who injects an “additive” on demand.

The most desirable is epidural anesthesia, which is administered during preterm labor if the child’s condition is stable. She allows the woman in labor to relax and the birth process goes faster. At first birth, when the pain is stronger and the process lasts longer, the need for relaxation with the use of epidural anesthesia is also quite common.
Regional anesthesia also helps with the discoordination of labor, with a sharp increase in pressure in a woman, during natural childbirth, if the baby is large or giant, or during childbirth twins. Difficult and prolonged labor and seldom do without such analgesia, it gives relaxation, and it helps cervical dilatation.
At the onset of the stage, the attempt is usually not prescribed epidural anesthesia. Its main task is to facilitate the opening of the neck, and when the attempts began, there is no longer any need for this - the neck is fully opened. In addition, a woman should push and act in close tandem with the obstetrician so that the baby is born faster and without negative consequences for the health of the woman herself and the baby.

For caesarean section
The average duration of a delivery operation is 25-45 minutes. The very fact of using epidural anesthesia will make the operation a little longer - for the duration of the latent period, until anesthesia is effective (15–20 minutes).
Since surgical delivery requires a deeper desensitization, before the anesthesia is administered, the anesthetist must be sure that his patient is feeling well. A woman is measured for pressure and heart rate. A special cuff that will continuously measure pressure in real time and output data to the monitor is fixed on the arm.

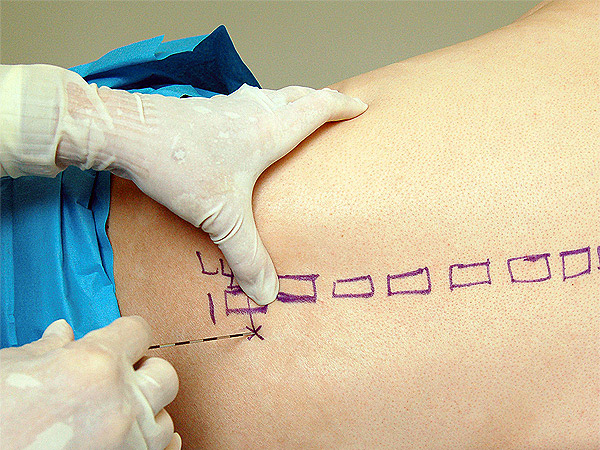
The position of the body with the introduction of tools in the spine will be the same as in natural childbirth - the woman will either sit or lie on her side. Right on the skin of the back doctor does the markup with a pencil. The vertebrae, between which the painkiller needle must be inserted for surgical delivery, are in the range between 2 and 5 lumbar vertebrae. The most acceptable puncture site is determined on the fact and on the spot.
As in the case of anesthesia during childbirth, the skin is subject to careful aseptic processing. A thin needle passes through the so-called yellow ligament between two vertebrae. As soon as the resistance becomes negative, the needle “falls”, a syringe with a catheter is attached to it. The lack of resistance on the other side of the needle will mean that the impact to the epidural space was successful.


The test dose is administered after hitting the desired point. About three minutes is the initial assessment of the effects of drugs. If the effect is there, the woman begins to feel numbness, and the main dose of drugs is slowly and smoothly administered to her.
Surgeons proceed to the operation after the appropriate command of the anesthesiologist. This specialist during the whole process of surgical delivery is next to the woman in labor, talks to her, adds the right amount of drugs through the catheter.
Support is provided until the operation completes. Throughout the cesarean section, the anesthesiologist and the midwife are closely monitoring the woman’s well-being.

All this time, a woman can see and hear everything that happens. This gives two excellent opportunities - to see how the baby is born and to attach the baby to the chest right in the operating room, which is extremely useful for the subsequent establishment of lactation.
When a woman is given epidural anesthesia before surgical delivery, the anesthesiologist is always ready for general anesthesia. This rule is. It may happen that the "epidural" will be held with an error, it will not work, and therefore at any time a specialist should be prepared to give a woman general anesthesia.

What does safety depend on?
The safety of a woman and her child depends on several factors. which makes sense to ask in advance, choosing one or another hospital:
- the skill level and competence of the anesthesiologist;
- the level of training and qualifications of obstetricians and surgeons;
- the presence in the obstetric institution of modern medical equipment (needles, dispensers, lumbar catheters, monitors);
- use in practice of modern and safe anesthetic drugs (Naropin, Bupivacaine);
- constant monitoring of the status of the mother and child.

Do not be shy of your own curiosity. When choosing a maternity hospital should ask all these questions. A woman has the full right to know which category of doctor will perform her operation or do anesthesia, is there any modern equipment in the maternity hospital and when was it last changed, which drugs are used for epidural anesthesia.

Why does it hurt anyway?
In their responses, many women note that they did not manage to completely get rid of all the unpleasant feelings after the epidural anesthesia. An official description of such cases and causes is included in the epidural anesthesia protocol, which is the main clinical recommendation for physicians. So, epidural anesthesia can be ineffective if:
- the operation began earlier than the full distribution of the drug in the epidural space;
- the initial dose of the drug was too low;
- mosaic blockade occurs (the drug is unevenly distributed, and one side is anesthetized, and the other is not, or partially loses sensitivity);
- individual lack of perception of the drug (it helps to change the drug to another);
- the young age of the patient (the ligaments in the spine are soft, therefore the anesthesiologist falsely treats them as an entry into the epidural space, loss of resistance).

Opinion of Dr. Komarovsky
The famous pediatrician Yevgeny Komarovsky has repeatedly stressed that epidural anesthesia is a very good modern method for reducing pain. It is highly effective and almost safe.
But the human factor is clearly manifested in it - if the anesthesiologist is skilled and qualified, the birth of the woman will be very comfortable and calm. If the specialist makes a mistake, epidural anesthesia can be quite dangerous for the mother and her baby.

Cost of
Often women are interested in whether such anesthesia is paid, whether it is necessary to pay extra for it separately. If childbirth takes place in a private clinic, under a medical services contract, the procedure is paid. The cost of it balances from 7 to 15 thousand rubles, depending on the region and on the particular clinic. The exact cost can be found out in advance, at the time of the conclusion of the contract for childbirth.
In state maternity hospitals and perinatal centers that receive women under the OMS policy, epidural anesthesia is completely free. It can be applied at any time of childbirth, at the request of the woman or the recommendation of a leading birth doctor.

Reviews
Opinions about epidural anesthesia in patients are quite different. One liked the effect during childbirth or caesarean section, while others complain about the side effects. Most of them note severe back pain, which disappear only a few weeks after childbirth.Others complain of headaches that have been haunting for several months, and still others claim that they practically did not experience a pronounced effect after an epidural injection in vaginal delivery.
After a cesarean section under regional anesthesia, according to reviews, the period of recovery from anesthesia is more gentle - it does not make you sick or sore. But there are also reviews with a description of the negative consequences - temporary or permanent paralysis of the limbs, which began after lumbar puncture.
In general, women who have tried various types of anesthesia on themselves due to circumstances tend to believe that epidural anesthesia is indeed the most benign and gentle of all.

About some of the nuances of the use of epidural anesthesia during childbirth, see the following video.



