Narrow pelvis during pregnancy and its clinical form
A narrow pelvis in a pregnant woman is one of the most extensive topics in obstetrics. The success of childbirth in the presence of such pathology is largely determined by the degree of education of the specialist in this matter, as well as his experience in assisting obstetric care for women suffering from this disorder.
If there are any anatomical parameters, the pelvis of a pregnant woman is considered narrow? What are its varieties and what should a woman know, who was given a similar diagnosis? We will understand in more detail.
What is a "narrow pelvis"?
Statistics show that approximately 5% of women in labor are diagnosed with various degrees of pelvic contraction. In order to clearly present all the features of this pathology, it is necessary to understand how the insufficient amount of some pelvic size can have on the normal course of the labor process.
In the second stage of labor, when the expulsion of the fetus occurs directly, the crumb must pass through the pelvic cavity.
If the shape, size or configuration of some bones relative to others do not correspond to the norm, then they create an obstacle to the normal generic patency of the child, which leads to the inevitable occurrence of problems at birth.

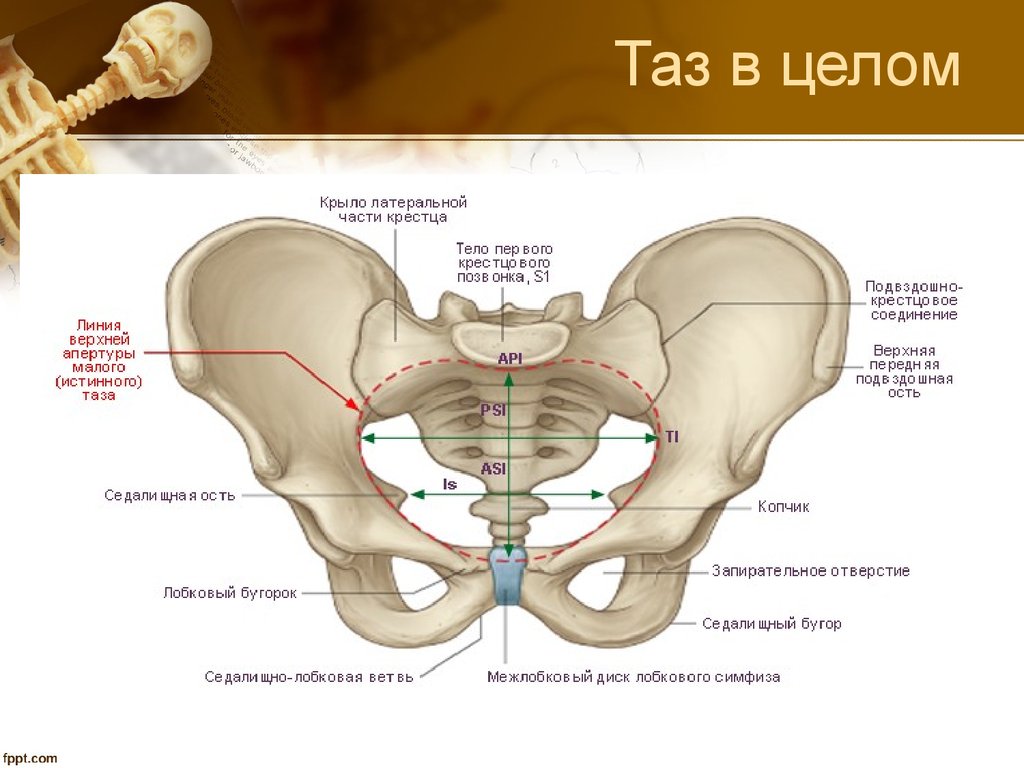
The small pelvis of a woman is a bone structure consisting of four components:
- 2 pelvic bones that are formed from the ileum, sciatic and pubic bones;
- sacrum;
- coccyx.
All these bone elements are interconnected by cartilage and ligaments.
In women, the size and shape of the pelvis is not the same as that of the stronger sex. In women, it is wider, but has less depth. Such gender characteristics are explained by female reproductive function.
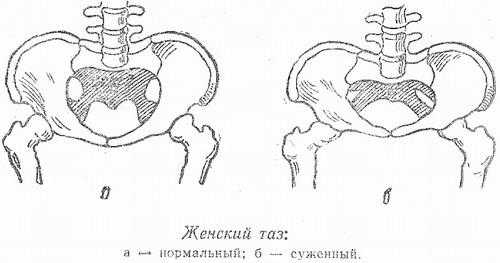
Conditionally pelvic narrowing is divided into two types:
- anatomical narrowing - the dimensions of one or several bones do not correspond to normal sizes);
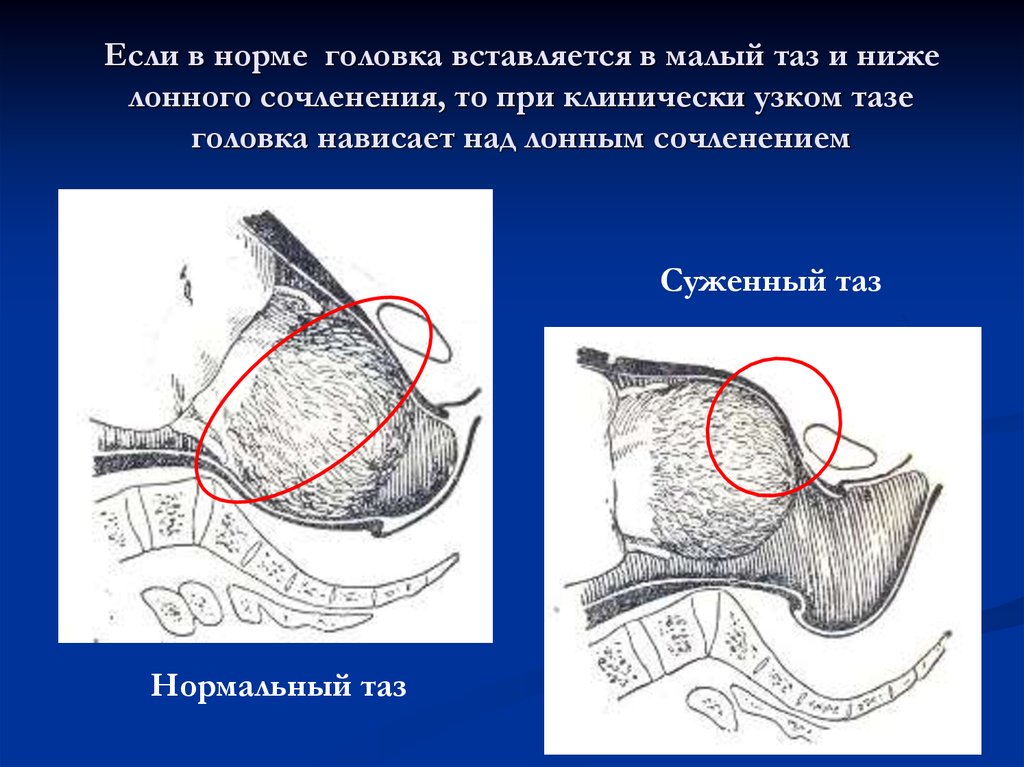
- Clinical (or functional) narrowing is a relative concept by which a pelvic size does not correspond to the size of the head of the fetus.
Even in the presence of a diagnosed anatomical narrowing, not all cases have a clinically narrow pelvis - for example, if the fetus has a relatively small weight, or, on the contrary, the anatomically normal pelvic size may have a clinical discrepancy with the large size of the child.
Causes of Contraction
The reasons for the development of this pathology vary depending on the type of narrowing: either it is an anatomical defect, or the mismatch of the size of the fetus relative to the size of the birth canal.
The following factors contribute to the formation of anatomical pelvic constriction:
- various reproductive dysfunctions;
- any irregular menstruation or too late the onset of menstruation;
- hormonal imbalance;
- infectious diseases;
- disproportionate exercise in childhood or adolescence, as well as a poor diet.
The above factors can have a negative effect on the formation of pelvic size.

Now let's talk about diseases that are directly the causes of such a pathology as anatomical narrowing.
These include:
- sexual infantilism (underdevelopment of the female reproductive system);
- delayed sexual development, triggered by various factors: neuroendocrine disorders, hereditary diseases, autoimmune processes, inflammatory diseases of an infectious nature, pituitary tumors, etc .;
- rickets (a disease predominantly of infants associated with insufficient intake of vitamin D, resulting in insufficient bone mineralization);
- osteomalacia, due to which bone tissue becomes too flexible;
- malignant bone formations;
- various forms of spinal curvature (kyphosis, lordosis, scoliosis);
- violation of the integrity of the pelvic bones due to injuries;
- Cerebral palsy;

- congenital features of the body structure associated with the hereditary factor;
- polio;
- exostoses (benign neoplasm of bone and cartilaginous nature, which is formed on the surface of the bone);
- birth trauma or damage caused in the prenatal period of development;
- acceleration (rapid increase in body length, with a significant lag in the formation of pelvic size);
- severe psycho-emotional stress (may trigger the development of “compensatory hyperfunction of the body”, as a result of which a contracted pelvis may form);
- intense sports in childhood and adolescence;
- violation of metabolic processes;
- insufficient or excessive production of female sex hormones;
- excessive content of male sex hormones.
Prevention or timely treatment of these pathologies reduces the risk of various disorders in the pelvic structure.


Classification
In clinical medicine, there are several classifications of anatomical pelvic constriction. The main one is based on morphoentgenological features.
Let us examine the varieties of such restrictions in more detail.
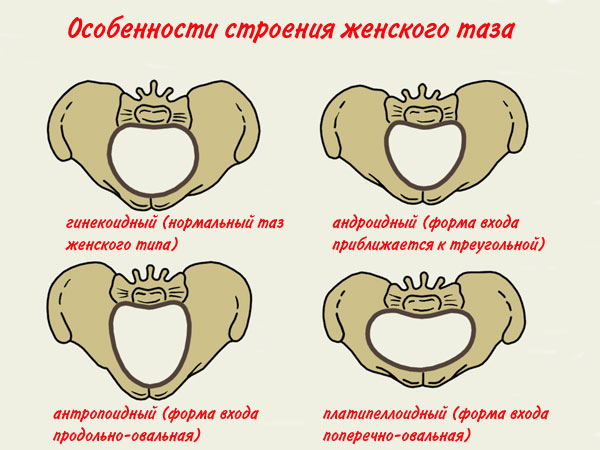
- Gynecoid type. Women with such a pelvic structure make up more than half of the total number of pregnant women. This type is a variant of the norm. Women of this type have bright gender characteristics: thin waist, wide hips, body weight and height fluctuate within averages.
- Android type. This kind of pathological narrowing occurs in every fifth woman in labor. From the name it follows that in this case the formation of the small pelvis occurs in the male type. It is characterized by the presence of a triangular entrance and a slightly smaller outlet. The owner of a similar pelvic shape is inherent in the structure of the body, similar to the male: unexpressed waist, massive shoulders, narrow hips, etc.
- Anthropoid type. A characteristic feature of this restriction is the size of the direct size of the entrance and the transverse size of more than normal values. Expectant mothers with a similar defect have a tall, thin-bodied physique, narrow hips, and massive shoulders.
- Platypeloid type. This form of constriction is less common. In this case, the pelvis has a flattened shape from top to bottom. Also the sacrum here is slightly deflected from behind. Women with this type of constriction are characterized by high growth and thinness. They have poorly developed muscles and poor skin elasticity.
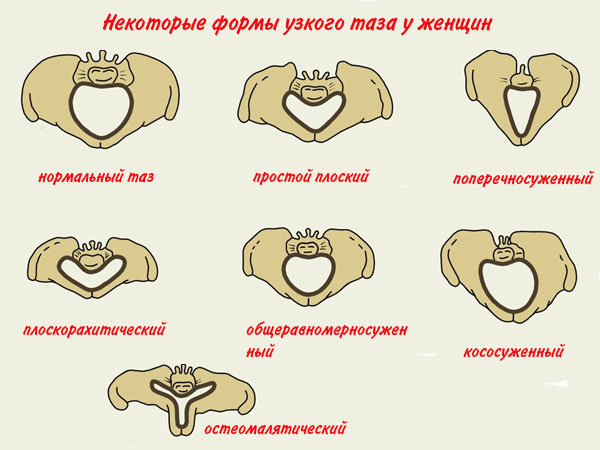
Types of Krassovsky
In addition to this classification, there are varieties of the constricted pelvis "according to Krassovsky". The following types are distinguished:
- General uniformly constricted. The shape of the pelvis is normal, but all the sizes of the bones are reduced in the same proportions by about 1.5 cm. This form of contraction is inherent in women with an average height and normal physique.
- Cross-coned (Robertovsky). This type of narrowing is characterized by a shortening of the transverse dimensions of about 1 cm, as well as a relative decrease or increase in the straight diameter of the entrance. This type of pelvis is found in the fair sex, folded by a male type, often suffering from hyperandrogenism - increased production of male sex hormones.
- Flat pelvis. There are the following types:
- simple flat - in this case there is a decrease in the size of straight diameters, and the transverse diameter of the entrance, on the contrary, is greater than the clinical norm
- flatrakhitichesky - characterized by a narrowing of the direct diameter of the entrance and an increase in all other direct diameters, and the sacrum in this case has a flat shape;
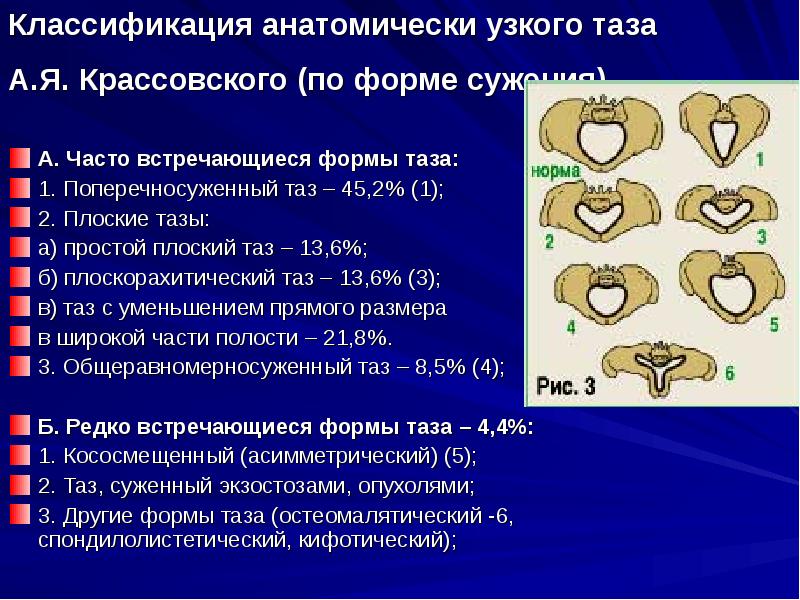
- Offset (asymmetric). The formation of this rather rare form of narrowing occurs due to diseases suffered during childhood or adolescence or due to injuries such as rickets, dislocation of the hip joint, incorrectly accreted fracture of the femur).
- Deformity of tumors. Damage to the pelvis may be due to the occurrence of tumors, exostoses, that is, a benign growth of bone and cartilage tissue.
- Funnel-shaped - A similar violation occurs on the background of some hormonal disorders. The main feature is the narrowing of the output from top to bottom in the form of a funnel).
- Kyphotic. Refers to the type of funnel. Due to the deformation of the spinal column, the center of gravity of the body is shifted slightly forward.
- Spondylolisthetic. The direct size of the entrance is insufficient due to the displacement of the V lumbar vertebra from the base of the sacral bone.
- Osteomalactic. This type of narrowing is formed gradually in women of reproductive age. Deformation of bone tissue due to osteomalacia leads to a pronounced curvature of the pelvis. First, the spinal column is affected, then the pathological process spreads to the small pelvis, chest and limbs.
Degrees of contraction and measurement
The diagnosis of a “narrow pelvis” is made by an obstetrician-gynecologist based on the results of measuring the main obstetric parameters of the pelvis of a pregnant woman.
If any of these parameters do not correspond to the indicators adopted by experts for the average statistical norm, then this will speak about a certain form of narrowing, which is perceived as pathology.
With an objective assessment of the pelvis, the doctor measures the following parameters.
Lumbosacral rhombus or Michaelis rhombus
When a woman is standing, this diamond becomes clearly visible in the lower back. The obstetrician measures the distance between its opposite extreme points. The distance between the vertical points in the norm should be not less than 11 cm, and between the horizontal - not less than 10 cm.

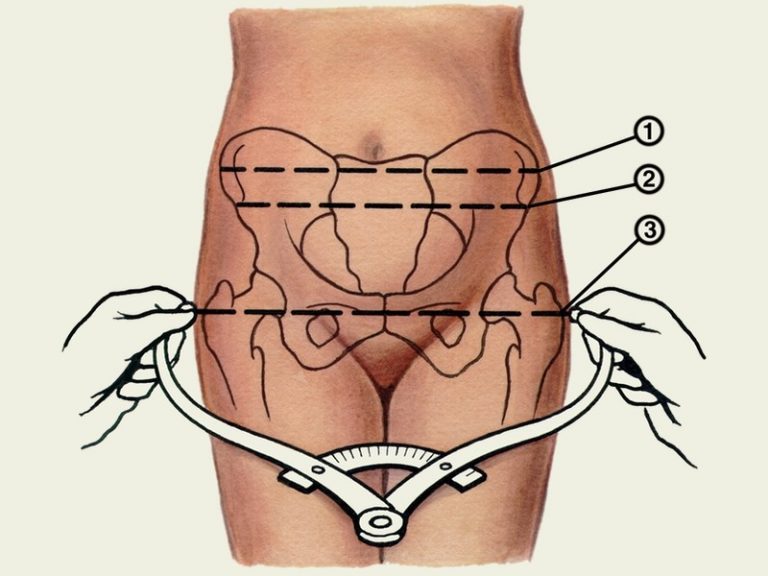
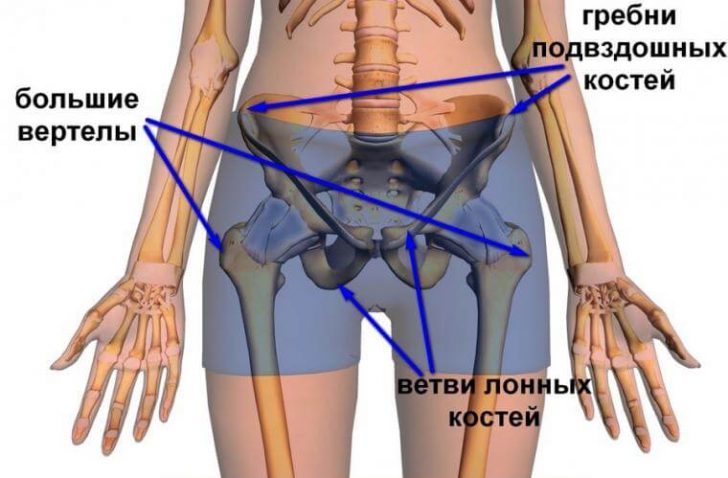
Interosseous size
To determine this indicator, a woman must lie on the couch. In this position, the obstetrician determines the distance between the two tubercles of the iliac bones. Normally, this size should be at least 25 cm:
- The maximum distance between the iliac bones. Measurement takes place in the supine position. The distance between the most distant points on the ilium is determined. This size must be at least 28 cm.

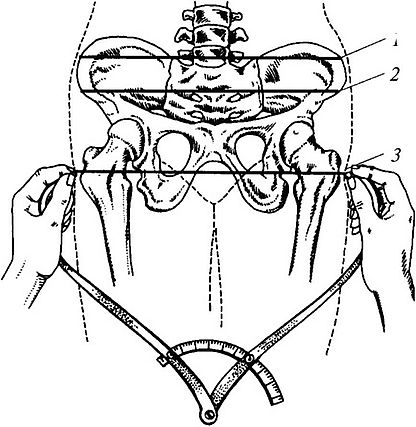
- The distance between the big skewers. In order to take a measurement, a woman must lie down on a couch and bend her legs. The distance between the upper ends of the femurs is determined here. Normally, this figure is 30 cm.
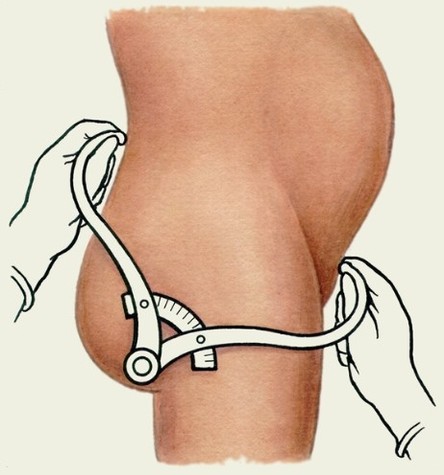
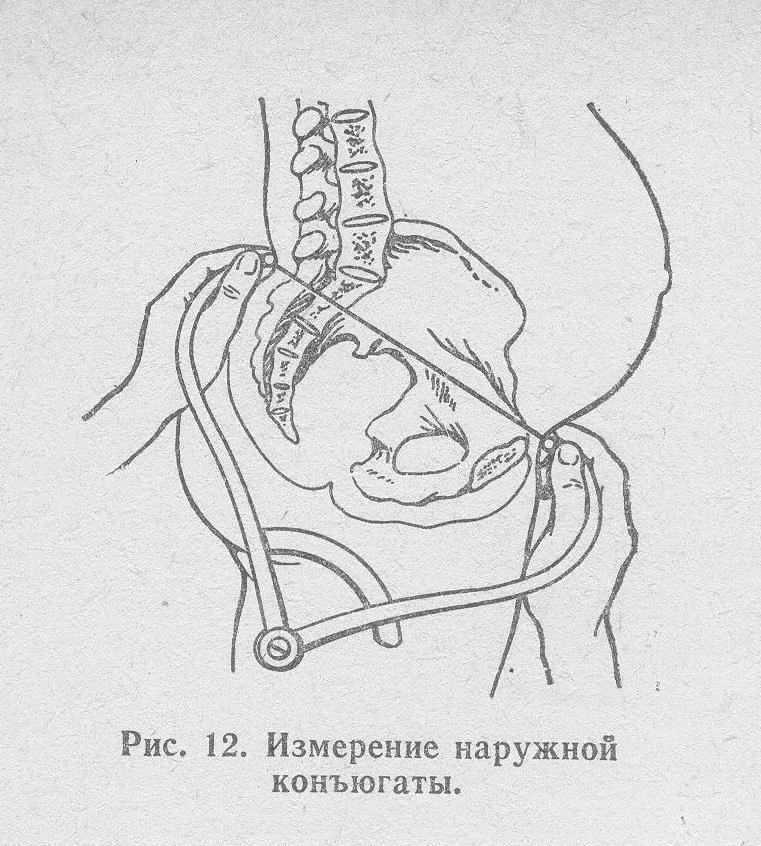
Conjugate external
To determine this indicator, a woman needs to lie on her side, while the upper leg must be straight and the lower leg must be bent.
The midwife measures the distance between the top of the Michaelis rhombus and the upper nearby point of the pubic symphysis. Normally, the outer conjugate should be at least 20 cm.
Conjugate lateral
Measured when a woman is lying on her side. In this case, the ends of the tazomer are applied to the anterior and posterior points of the upper zone of the Ilium, left and right. Normally, this value should not be less than 14 cm.

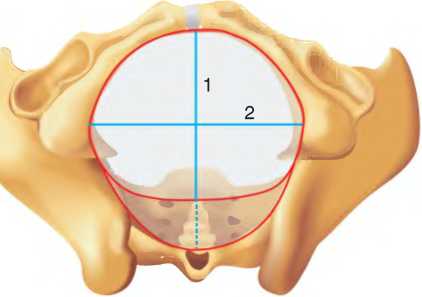
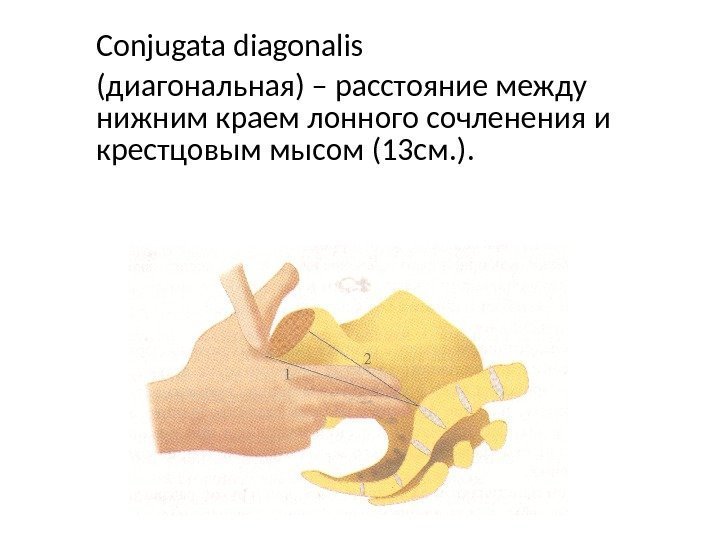
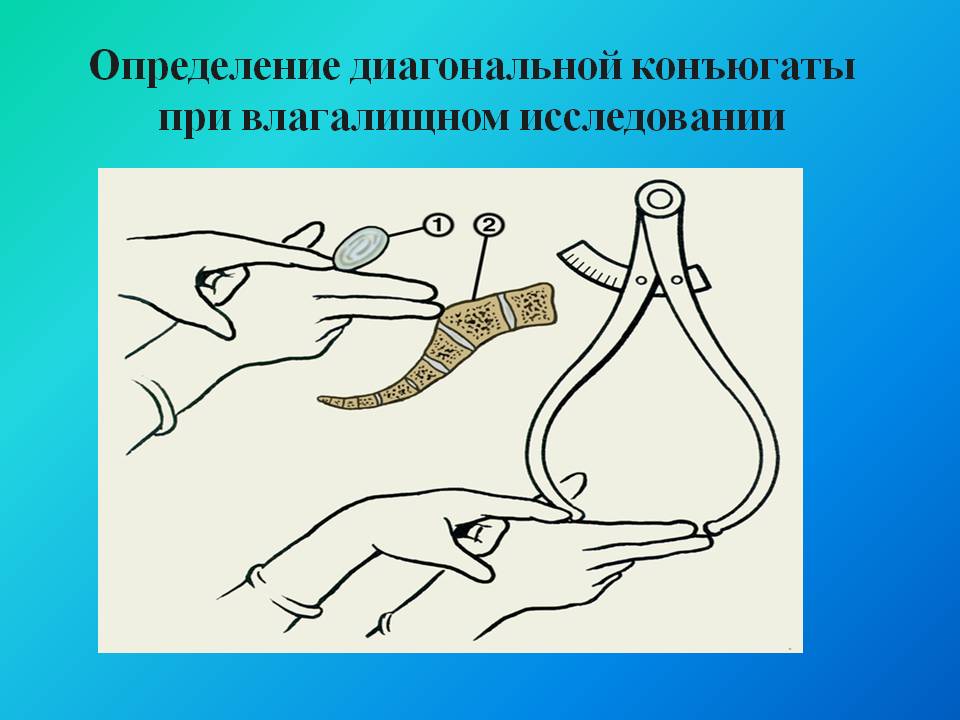
True conjugate
This indicator can be measured only during vaginal examination. Currently, the definition of true conjugates is not mandatory for all expectant mothers.Based on the measurement of this size, one can judge the degree of pelvic constriction. Normally, the true conjugate should be 11 cm.
If any of the listed indicators does not comply with the generally accepted norm, the obstetrician diagnoses an anatomically narrow pelvis for a pregnant woman. Statistics indicate that various types of narrowing occur in 10% of women who have registered for pregnancy.
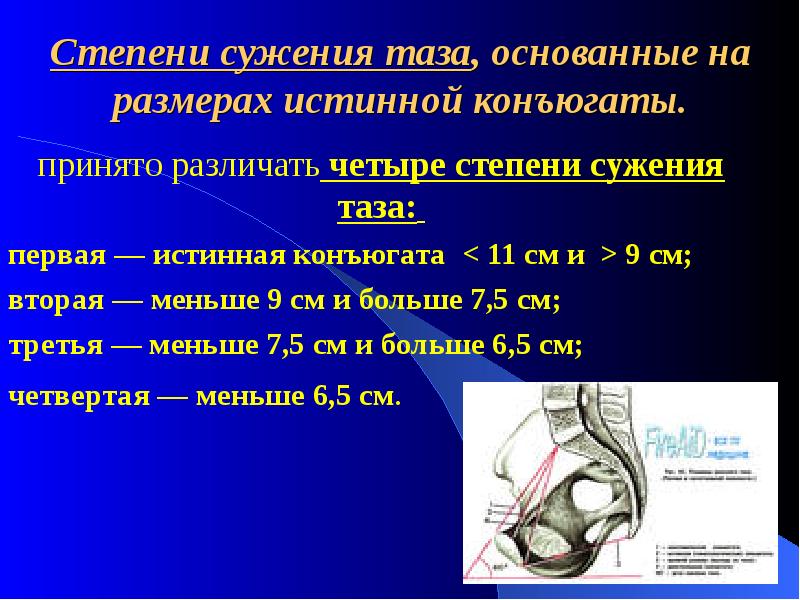
As already mentioned, the degree of narrowing can be determined by changing the true conjugates. Experts distinguish several degrees of pelvic constriction (depending on how short the size is), which are displayed below:
- 1 degree - IP = 10 cm;
- 2 degree - IP = 8.5 - 9.9 cm;
- 3 degree - IP = 5 - 8.4 cm;
- 4 degree - IP = less than 5 cm.
In clinical practice, the restriction of 1 and 2 degrees is considered to be conditional, since there is no guarantee that such a pathological deviation will make it difficult during pregnancy or during childbirth.
Grade 3 and 4 narrowing is an infrequent phenomenon in obstetric practice, usually found in women who have suffered serious injuries or diseases of the musculoskeletal system.
Diagnostics
The assessment of the pelvis of a pregnant woman is carried out on the day of her registration in the antenatal clinic. In order to identify possible violations of the normal structure of the pelvis, The gynecologist should conduct the following diagnostic procedures:
- history taking;
- Objective examination of the patient, which includes anthropometry, inspection, measurement of pelvic size and, if necessary, vaginal examination.
In special cases, the specialist may resort to additional diagnostic methods, which include ultrasound and X-ray diffraction.
During the procedure of taking anamnesis, it is necessary to pay attention to the diseases and life conditions suffered by the woman in which she was in childhood and adolescence. This information may indicate the cause of the violation of the pelvic structure.
In addition, the gynecologist can get information that will be very useful for managing this pregnancy - for example, when a woman has a menstrual cycle, as previous births have taken place, they were complicated by any pathologies, which resulted in, etc.


An objective study of a pregnant woman begins with an external examination. The specialist draws attention to the constitution of the body. There are several conditional criteria for the anthropometric features of the patient, which may indicate a probable contraction. Among them:
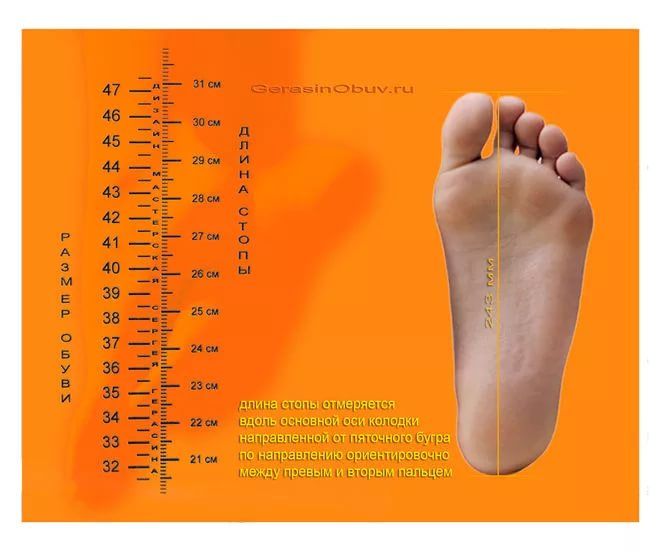
- short stature (less than 160 cm);
- small foot size (less than 36);
- the index finger is shorter than 8 cm, and the length of the brush is less than 16 cm;
- hip circumference less than 85 cm;
- Solov'ev index - measured wrist circumference at the level of prominent condyle of the forearm. Assessing this figure, a specialist can judge the degree of bone thickness. Normally, the Solovyov index should be 14.5-15 cm;
- external signs of hyperandrogenism: excessive body hair, as well as male-type hair growth, unexpressed hips and waist, broad shoulders and neck, small breasts, etc.
In addition, the gynecologist can be examined abdomen, the shape of which can also indicate some deviations from the norm.
The physician should pay attention to the nature of the gait, which changes may indicate various kinds of disorders in the locomotor system of a pregnant woman.

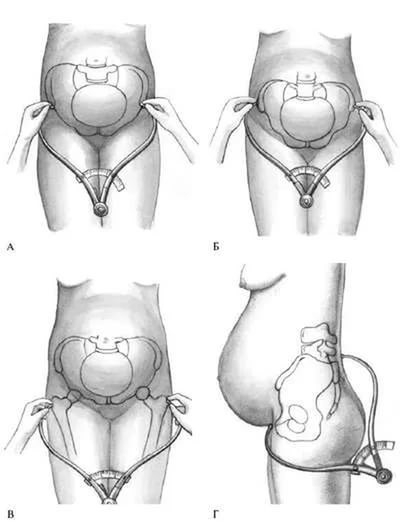
A crucial role in establishing the diagnosis is the measurement of its basic dimensions with the help of a special device - the tazomer. By its design it resembles a compass with rounded ends and is used exclusively in obstetrics.
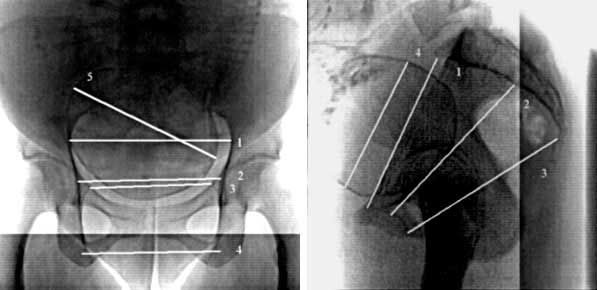
Roentgenopelviometry is carried out for special reasons at a time not earlier than 37 weeks of pregnancy. Also, this diagnostic study can be carried out in childbirth.
X-ray diopiometry makes it possible to determine the morphology of the pelvic walls, the shape of the entrance, the degree of inclination of the pelvic walls, the structural features and location of the ischial bones and the curvature of the sacrum. In addition, a similar method of instrumental diagnostics allows calculating all pelvic diameters, detecting the presence of tumors, determining the size of the baby’s head and its spatial position.
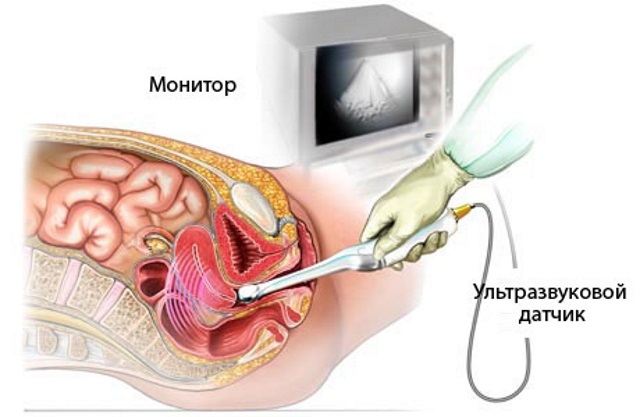
Using ultrasound, you can calculate the value of the true conjugates, the position and size of the fetal head, as well as the nature of its insertion into the entrance.
Using a transvaginal transducer makes it possible to measure all the pelvic diameters of a woman.
Tactics of pregnancy
If a narrow pelvis is diagnosed to a pregnant woman, further actions of the pregnancy doctor suggest that the following measures should be taken.
With the established narrowing, the mechanism of delivery is determined taking into account the degree of narrowing and the size of the fetus. Most often, doctors prefer to play it safe and choose a cesarean section in this case.
Considering the fact that women with pelvic constriction quite often give birth before the date of expected birth, It is advisable to hospitalize such a patient in advance to avoid the development of various complications.
Childbirth in a natural way is acceptable for women in labor with 1 degree of narrowing and with a mass of the fetus not more than 3 kg 500g.

In all other cases, gynecologists, based on clinical experience, do not advise women to give birth independently. Therefore, their urgent recommendations will be associated with the planned caesarean section after the fetus achieves normal gestational development. This tactic makes it possible to significantly reduce the risk of severe damage to the birth canal of a woman and traumatizing the fetus during natural childbirth.
Read more about the size of the female pelvis in the next video.









